
By L. Richardson
Key Takeaways
Recent research reveals alarming risks of high-potency cannabis use among teenagers, with major consequences for mental health, brain development, and public policy.
• High-THC cannabis doubles psychosis risk: Study of 463,396 teens shows a 2.19x greater risk of psychotic disorders and a 2.0x greater risk of bipolar disorder from cannabis use (relative risk; for example, if the baseline risk of developing a psychotic disorder by age 26 is about 1 in 200, cannabis users would face a risk closer to 1 in 90).
• Brain development severely impacted: Cannabis use causes measurable brain shrinkage, particularly in prefrontal regions, and arrests development until age 25-26 (Owens & al., 2022)
• Pregnancy creates generational harm: THC crosses the placenta and enters breast milk, causing fetal brain changes linked to autism and ADHD in offspring (Ryan et al., 2024)
• Modern potency levels unprecedented: Today’s cannabis contains 20%+ THC versus 2-4% historically, with concentrates reaching 95% concentration (Thakrar & Rastegar, 2021)
• Corporate interests drive normalization: Cannabis industry spent $31+ million lobbying in 2021, replicating tobacco industry tactics to maximize youth consumption (Rotering & Apollonio, 2022)
• Policy action urgently needed: States should implement potency caps, youth marketing bans, and treat high-THC products as a public health crisis requiring instant intervention. Concrete activist actions can make an immediate impact: Contact your state legislators to demand laws restricting cannabis potency to 15% THC or lower. Organize or join rallies at your state capitol calling for stronger youth protections and stricter advertising restrictions. Draft and circulate petitions within your local community, urging school boards to add high-potency cannabis dangers to drug education programs. Form neighborhood parent groups to share fact sheets and host informational meetings, increasing grassroots pressure on policymakers. Volunteer with organizations that lobby for public health-focused cannabis regulation. Every call, petition, rally, and conversation increases the momentum for urgent reform.
The transition from cigarette to cannabis use among young Americans represents a shift from stimulating to sedating substances at (Eser, 2026) a critical time when mental lucidity and development remain crucial for healthy brain maturation. (Longitudinal trends in the past 30-day co-use of nicotine/tobacco, alcohol, and cannabis among youth and adults in the PATH study, 2026) Teen Cannabis Psychosis Risk has reached crisis levels. Teenagers who use cannabis face twice the risk of developing psychotic and bipolar disorders, according to research. About 26% of twelfth graders report past-year cannabis use, and our youth face danger due to THC levels exceeding 20% while concentrates reach 95%. ((NIDA), 2024) Cannabis use preceded psychiatric diagnoses by an average of 1.7 to 2.3 years. (Large et al., 2011, pp. 555-561) This reveals a disturbing pattern we can no longer ignore. We’ll get into the scientific evidence behind Adolescent Marijuana Psychosis and High THC Mental Health Risks, expose how this threatens our heritage, and rally for constitutional action to protect our heritage from this assault on youthful minds.
II. The Scientific Siege: Unveiling the Dangers to Our Progeny
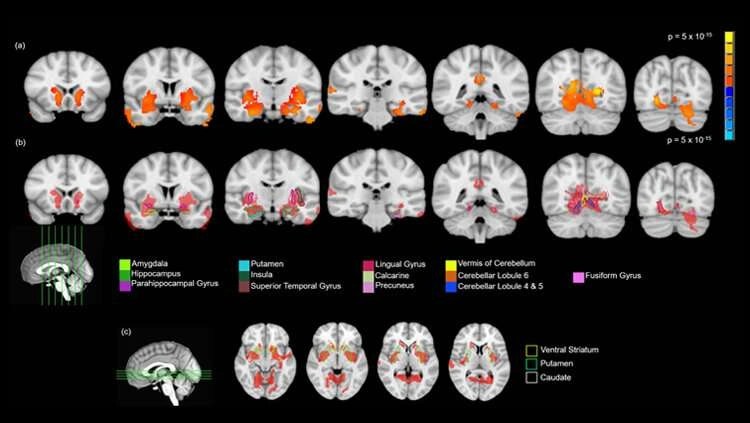
Image Source: Medical Xpress
Longitudinal research spanning the last decade has produced findings that expose the full scope of what high-potency cannabis inflicts upon developing minds and future generations (Hines et al., 2020, pp. 1044-1051). The scale of these studies, combined with the accuracy of clinical health records, removes any doubt about the trajectory we face when our youth encounter THC concentrations that previous generations never imagined. (Aks et al., 2025)
JAMA longitudinal thunder (463,396 teens, THC >20%/95% concentrates, precedes diagnoses by years)
A landmark investigation published in JAMA Health Forum tracked 463,396 adolescents ages 13-17 through age 26. This created one of the most complete datasets on Adolescent Marijuana Psychosis ever assembled [1]. Past-year cannabis use through this developmental phase was associated with a 2.19 times greater risk of developing psychotic disorders and 2.0 times greater risk of developing bipolar disorder [1]. While these outcomes show a strong association, it is important to acknowledge that, as with most observational studies, there may be unmeasured confounding factors that affect both cannabis use and the risk for psychiatric disorders. Although the researchers rigorously excluded adolescents with pre-existing symptoms and adjusted for known confounders, causation cannot be definitively established from correlation alone. Yet even in the presence of scientific uncertainty, the scale and effects of these results require urgent action. The potential for (Cannabis Use and Earlier Onset of Psychosis: A Systematic Meta-analysis, 2007, pp. 480-487) life-altering mental illnesses among our young warriors, combined with the swift escalation in cannabis potency, means that waiting for absolute certainty would be reckless. The precautionary principle compels us: when the risks to our youth and heritage may be severe and irreversible, even possible dangers justify immediate preventive measures (Hines et al., 2024). We must not allow uncertainty to paralyze us; instead, treat these data as a clear signal for strong, immediate prevention efforts.
Depression alone increased by one-third among cannabis users. Anxiety rose by about a quarter [1]. The researchers excluded adolescents who had symptoms of mental illnesses before using cannabis. This established that these teens were developing psychiatric conditions after their exposure began [1]. Cannabis use preceded psychiatric diagnoses by an average of 1.7 to 2.3 years, supporting a contributory role rather than reverse causation [1][2].
The timing matters. We’re no longer dealing with the marijuana of decades past, when THC content ranged from 2% to 4%. The typical average THC content of cannabis flower in Northern California, where this study took place, now exceeds 20% [1]. Concentrations reach even more alarming levels. Some products deliver 70% to 90% THC, and certain forms approach 95% [2][3]. These products act on cannabinoid 1 receptors, which are highly expressed in the adolescent brain. They disrupt neurodevelopment inside regions related to motivation, emotional processing, and affective functioning [1].
Nearly 4,000 teens in the study were diagnosed with psychotic or bipolar disorders [1]. This represents a small fraction of the total cohort. The implications reach way beyond private tragedy. The social cost of schizophrenia has been calculated at $350 billion annually [1]. We could wipe out the entire economic value of the cannabis market by increasing the number of people who develop this condition in a preventable way [1].
Up to one-third of European adolescents ages 12 to 17 smoke cannabis, with 1.2% consuming it regularly [4]. American high school teens show progressive increases from 14% to 44% [4]. A Canadian Cannabis Survey reported that youth ages 16 to 24 cons (European Drug Report 2025: Trends and Developments, n.d.)umed cannabis at twice the rate of older people. 31% of those aged 16 to 19 and 20 to 24 report (Reported Drug Use Among Adolescents Remained Low in 2024, 2024)ed increased consumption due to COVID-19 [4]. Fewer participants believed daily cannabis smoke increases vulnerability for mental health disorders, dropping from 75% in 2019 to 66% in 2020 [4]. This is concerning.
Chronic cannabis exposure before age 17 induces long-lasting neurocognitive decrements in IQ, working memory, executive functioning, decision making, impulsivity, attention, and scholastic performance [4]. Young subjects consuming high-THC cannabis strains were (A Fine-Grained Longitudinal Study of Adolescent Cannabis Use and Its Relation to Cognitive Performance in Young Adulthood, 2025) more likely to develop anxiety and cannabis use disorder, experience psychiatric-like symptoms, and suffer frequent relapses [4]. Chronic THC exposure during adolescence disrupts sensorimotor gating substantially. This effect was neither observed directly after adolescent THC exposure nor when THC was administered to adult rats [4].
Magnetic resonance imaging studies with 1,598 scans from 799 participants showed that cannabis use was associated with accelerated age-related cortical thinning from ages 14 to 19. This occurred predominantly in prefrontal regions [5]. Greater cannabis use was associated with increased thinning in left and right prefrontal cortices in a dose-dependent fashion at five-year follow-up [5 (Albaugh et al., 2021, pp. 1036-1045)]. These spatial patterns of cannabis-related thinning aligned with cannabinoid 1 receptor-binding maps [5]. The prefrontal cortex, which is involved in executive functioning, may not fully develop until around age 25 [6]. Thinning in this region was associated with more attentio (Tamnes et al., 2010, pp. 534-548)nal impulsiveness at follow-up [6]. For example, teens regularly using high-THC cannabis scored lower on executive function tests such as the n-back working memory task, showed poorer performance on response inhibition measured by the Go/No-Go test, and exhibited higher impulsivity and reduced ability to delay gratification. These deficits in working memory, impulse control, and decision making highlight how cannabis exposure can concretely disrupt the developmental milestones essential for mature executive function.
02
Research demonstrates that THC causes shrinkage of dendritic arborization, the neurons’ network of antennae critical for communication between neurons [6]. This results in atrophy of certain cortical regions during brain maturation [6]. THC alters the expression of genes that regulate the structure and function of synapses and dendrites. This leads to dendritic arbor atrophy, causing cortical thinning [6].
pregnancy perils: Fetal harm from cannabinoids, lifelong effects on future bloodline
Cannabis use during pregnancy may affect fetal development and create pregnancy complications that resound throughout generations. The chemicals in cannabis, particularly THC, pass through the maternal system to the baby and may harm developmental processes [7]. THC is lipid-soluble, crosses the placenta, and transfers into breast milk [7]. Fetal THC concentration has been reported at 10% of maternal concentration. The risks of adverse outcomes increase in a dose-dependent manner [7].
The prevalence of cannabis use among pregnant persons ranges from 3.9% to 16.0%. Usage reaches 43% among young adults aged 19-22 years [7]. The highest frequency occurs in the first trimester, when many patients report using cannabis to curb pregnancy-related nausea and vomiting [7]. Cannabis use during pregnancy has increased in the last 20 years, with reported rates varying between 3.9% and 22.6% in high-income countries [7].
Cannabis exposure during pregnancy has been associated with low birth weight, small-for-gestational-age neonates, neonatal intensive care unit admission, and perinatal mortality [7]. Neonates exposed to cannabinoids in utero demonstrate altered arousal patterns, regulation, and excitability in the first month of life [7]. Prior studies indicate a possible risk for postnatal neurocognitive and behavioral dysfunction. This includes attention deficit disorders, behavioral and short-term memory challenges, and intellectual disabilities [7].
Cannabinoid use was associated with diminished cognitive functioning in verbal reasoning, language comprehension, and executive function, independent of tobacco and other drugs [7]. Adolescents and adults exposed to cannabinoids prenatally encounter an increased risk of developing substance use disorder or psychiatric disorders [7]. Cannabinoid receptors are present in the fetus as early as 5 weeks [7].
Oregon Health & Science University researchers using a non-human primate model found that exposing pregnant subjects to THC altered the placental and fetal epigenome. This included chemical modifications to DNA responsible for gene regulation and expression [1]. These changes to gene regulation are consistent with those seen in many common neurobehavioral conditions, including autism spectrum disorder [1]. Changes involved genes associated with autism spectrum disorder and attention-deficit/hyperactivity disorder [1]. (Tadesse et al., 2024, pp. 142-151)These conditions are linked to adverse health outcomes in childhood and adolescence. This includes poorer memory and verbal reasoning skills, as well as increased hyperactivity, impulsivity, and inattention [1].
Research in rodents showed that prenatal exposure to cannabis led to lasting effects on cognitive and memory functions [2]. These effects are sex-specific, suggesting males and females may be affected differently by cannabis exposure in the womb [2]. Prenatal THC exposure impacted offspring’s desire to socialize, memory of previous social encounters, and learning capabilities in both males and females [2]. THC affects the fetal endocannabinoid system, a key player in fetal and adolescent neurodevelopment as well as cognitive and affective processing [2]. This disturbance leads to deficiencies in vital fatty acids, such as DHA and ARA, which may cause lifelong health problems [2].
Female offspring showed very active brain activity in the ventral hippocampus, which is involved in emotion and memory. Males showed less active brain activity in this same area [2]. Both male and female offspring showed cognitive deficits, but the mechanisms differed between sexes [2]. Cannabis use has been shown to remain or increase during the postpartum period [7]. (Sarikahya et al., 2023, pp. 4234-4250)
Cannabis smoke contains many toxic and cancer-causing chemicals found in tobacco smoke [7]. THC may be passed to infants through secondhand smoke [7]. Studies suggest cannabis use by women duri (Cannabis and Secondhand Smoke, 2024)ng pregnancy could be linked to problems with attention, memory, cognitive skills, and behavior in their children later in life [7]. Chemicals from cannabis can be passed to a baby through breastmilk. Because THC is stored in body fat and released slowly over time, a baby could still be exposed even after a woman has stopped using cannabis [7].
Dr. Amen’s arsenal: Brain shrinkage, testosterone crash, autism/dementia spikes
Dr. Daniel Amen’s research using single photon emission computed tomography (SPECT) imaging demonstrated abnormally low blood flow in virtually every area studied in nearly 1,000 marijuana users compared to healthy controls [3]. Areas known to be affected by Alzheimer’s pathology, such as the hippocampus, showed particularly compromised blood flow [3]. Low blood flow in the hippocampus distinguished marijuana users from controls reliably [3].
Marijuana is thought to interfere with memory formation by inhibiting activity in the hippocampus [3]. The global reduction in blood flow in marijuana users’ brains, with the hippocampus as the most affected region due to its function in memory and Alzheimer’s disease, suggests troubling effects that may be harbingers of brain damage [3]. This work indicates marijuana use has damaging influences on the brain, particularly regions important in memory and learning [3].
Cannabis arrests brain development in teens and young adults [3]. Teenagers and people in their 20s who use it have a higher incidence of anxiety, depression, suicide, and psychosis [3]. When young people start using marijuana or other drugs, their development gets arrested [3]. The brain doesn’t finish developing until age 25 or 26. Hurting it early might mean it never catches up [3].
Middle-aged folks and seniors whose weed use lands them in the hospital face elevated dementia risk within years. An emergency room visit or hospitalization due to cannabis use is associated with a 72% increased risk of a dementia diagnosis within five years compared to the general population [7]. These individuals also have a 23% increased risk of dementia within five years compared to people receiving hospital care for any other reason [7].
More than 16,000 people from a cohort of 6 million individuals aged 45 and older required hospital care due to weed use between 2008 and 2021 [7]. The annual rate of first-time hospital visits for weed use increased more than fivefold during the study. It rose from about 7 people per 100,000 in 2008 to nearly 38 per 100,000 in 2021 [7]. About 5% of those hospitalized for weed use developed dementia within five years, and 19% did so within 10 years [7]. Under 4% of those hospitalized for other health problems developed dementia within five years, and 15% within 10 years, by comparison [7]. Slightly over 1% had a dementia diagnosis within five years in the general population, and nearly 6% within 10 years [7].
Long-term and heavy cannabis use has been associated with memory problems in midlife, along with changes in brain structure associated with dementia [7]. While some research suggests that regular cannabis use might directly increase dementia risk through changes in brain structure, the long-term relationship is still being investigated and is not fully settled. It is important to acknowledge that heavy cannabis users may also face higher rates of other established dementia risk factors, such as high blood pressure, head trauma and other injuries, depression, and social isolation [7]. These accompanying risks could contribute to or compound dementia outcomes. Recognizing such uncertainties in the science reinforces the vital need for more rigorous research, even as existing evidence points to serious cause for concern.
Cannabis use in individuals with autism spectrum disorder presents particular vulnerability to pro-psychotic effects of cannabinoid exposure, which may be passed on to their own children [4]. Cannabis exposure among individuals with autism spectrum disorders
III. Social Trends: Cannabis and Its Role in Population Health
American substance use changed fundamentally between 2021 and 2023. Cannabis-only use surged from 7.2% to 10.6%, overtaking cigarette-only use, which declined from 10.8% to 8.8% during the same period [1]. This represents more than a public health trend. It signals a considered replacement of one substance with another, trading the stimulating properties of nicotine for the sedative effects of high-THC cannabis at a time when our nation faces threats requiring watchfulness, not passivity.
Plato’s Republic: Weed as a modern “vegetarian diet” sapping thymos for harmonious control
Plato understood that spiritedness, what the Greeks called thymos, drives men to defend their communities, assert their worth, and resist subjugation. In his Republic, he described how certain diets and substances could dampen this vital force, rendering guardians docile and unsuited for their protective duties. Cannabis functions as a modern equivalent to those ancient pacifying regimens, chemically suppressing the assertive drive our young men need to defend sovereignty and bloodline. We can see this loss of thymos reflected in contemporary youth culture, where issues like declining participation in team sports, lower rates of community service, and an epidemic of social isolation are matched by rising rates of cannabis use. Viral trends online often glorify passivity and escapism over purposeful action and civic engagement, while the normalization of high-THC products in social circles dulls the spiritedness once seen in youth-led movements or activism. The same force that led past generations to demand justice or rally to their communities is being quietly replaced by disengagement, retreat into digital worlds, and an absence of the assertive ethos needed to protect our heritage. Activists must recognize this connection and work to restore thymos by encouraging real-life challenges, leadership, and community involvement as antidotes to the apathy spreading through today’s adolescent ranks.
The pharmacological mechanism operates through cannabinoid receptors that regulate motivation, emotional processing, and the very circuits governing spirited action. Nicotine heightens alertness and focuses attention, creating sharper warriors capable of rapid decision-making. THC induces compliance and passivity. The contrast appears stark when we examine usage patterns: cannabis-only use predominates among socioeconomically advantaged groups, including college-educated, high-income, and privately covered individuals, while cigarette-only use remains most prevalent among socioeconomically disadvantaged adults with lower education, income, or lacking insurance [1].
This inversion matters. Those with resources and education, the natural leadership class who should be most vigilant against threats to our heritage, instead consume substances that dull their protective instincts. By the same token, one in four adults calling tobacco quitlines to improve their health reported past-30-day marijuana use, and 43% of these co-users expressed interest in quitting or cutting down their cannabis consumption [2]. They recognize, dimly, that something has compromised their vitality.
Raw Egg Nationalist’s manifesto: Surging pot replaces nicotine’s fire, infiltrates foods like corn/soy poisons—corporate plot breeding submissive, unhealthy masses unfit for sovereignty
Raw Egg Nationalist identified a pattern of corporate control that goes far beyond cannabis itself. He describes people unable to captain their personal destinies, bereft of traditional social and cultural institutions that offer aid when those destinies prove ill-starred [3]. The neoliberal project effected a momentous change toward greater social inequality and the restoration of power to the upper class, felt by ordinary folks as a wholesale assault on their security and dignity [3].
Cannabis legalization fits into this system. Elites promote a Great Reset in which corporations own everything and ordinary people own nothing [3]. Anything plebeians need, from shelter to transportation, they will rent. And as they await their next dispatch of necessities, they will nourish themselves on soy nuggets, cricket crisps, and other sustainable noshes while cannabis keeps them compliant [3].
Hemp and cannabinoids have already begun infiltrating food products under regulatory systems that permit their presence while restricting others. Hemp containing a concentration of not more than 0.3% THC on a dry weight basis is allowed as an ingredient in meat, poultry, and egg products [8]. Hemp-seed oil and seeds from industrial hemp may be used in these products in lieu of other edible seeds and oils for flavoring purposes [8]. These low-THC limits notwithstanding, the normalization of cannabis-derived ingredients in everyday foods resembles the corporate strategy that filled processed products with corn syrup and soy derivatives, creating populations plagued by obesity, metabolic dysfunction, and diminished physical capacity.
The regulatory apparatus prohibits cannabis containing more than 0.3% THC as an unapproved food additive that adulterates products [8]. Yet the very fact that regulators have to handle these boundaries reveals how the industry pushes to expand cannabis presence in the food supply. The marijuana and cannabis industry spent over $4.2 million lobbying on issues and legislation in 2021, including the Marijuana Opportunity, Reinvestment and Expungement Act [5].
Organizations spent a combined $31.1 million lobbying in 2021 on issues including the MORE Act [5]. The National Cannabis Industry Association spent $150,000 on lobbyists to promote cannabis legislation between April and December 2021, while the Minority Cannabis Business Association spent $40,000 on a single lobbyist and an additional $30,000 hiring the K&L Gates firm [5]. Canopy Growth Corp. hired two in-house lobbyists for $650,000 and spent $180,000 to hire K&L Gates for work on the MORE Act, the SAFE Banking Act, and general support for federal cannabis legalization [5].
This massive lobbying apparatus exists to create a for-profit production and sale model that damages public health, as the tobacco and alcohol industries showed [6]. Rather than adopt alternatives such as government monopolies in retail or supply, restricting sales to non-profit public benefit corporations, or grow-and-give models that prevent corporate predation, the emerging cannabis industry replicates the most exploitative commercial patterns [6]. In places like Uruguay and Quebec, however, policymakers have enforced strict THC potency caps—with Uruguay capping legal cannabis at 9% THC and Quebec banning cannabis products above 30% THC—which have proven effective in limiting access to high-potency products and curbing related health risks. We face not simply a public health crisis but a system designed to maximize consumption among at-risk populations.
The change in routes of cannabis use aggravates these concerns. 15.3% of adults reported current cannabis use in 2022, with 80% reporting smoking [9]. Eating, vaping, and dabbing—inhaling heated concentrated cannabis—were also common, and half of the respondents reported multiple routes of use [9]. Vaping and dabbing were most prevalent among adults aged 18-24 years [9]. Compared with 2016 data, the prevalence of eating and vaping marijuana was each higher in 2022, as was the prevalence of reporting multiple routes of use [9].
Dabbing often requires the use of a blowtorch, which increases risk for burn injuries [9]. This route delivers highly concentrated THC products that can trigger acute psychosis [9]. The wider availability of edibles has been associated with increased accidental pediatric ingestion [9]. Each delivery method serves corporate interests by creating new market segments and consumption occasions, transforming cannabis from an occasional indulgence into an omnipresent element of daily life.
Raw Egg Nationalist sees such developments as part of a wider assault where the body appears as the last redoubt for making a stand against commercial forces [3]. Its care and feeding become sacred doctrine, a path of redemption for individuals and their nations [3]. The fraught winter of 2020 saw one of the largest-ever transfers of wealth upward, with Federal Reserve actions advantaging the most powerful companies by $1.5 trillion [3]. Cannabis legalization occurred within this same timeframe, another mechanism by which elites extract wealth while rendering the population less capable of resistance.
ethnic replacement: Disparities fuel invasion, dulling our kin while elites prosper
The socioeconomic patterns of cannabis use reveal how this substance operates as a tool of ethnic replacement and population control. Cannabis-only use increased during 2015-2019, but the distribution remained uneven [1]. Cigarette-only use was most prevalent among socioeconomically disadvantaged adults, while cannabis-only use predominated among more socioeconomically advantaged groups [1].
This creates a pincer effect. Our most capable citizens, those with education and resources who should lead resistance to demographic replacement, consume cannabis that saps their thymos and dims their awareness of threats. Disadvantaged populations that bear the heaviest burdens of displacement continue smoking cigarettes, trapped in a different form of substance dependence while facing additional stigma and health consequences. The longitudinal research documented that ethnic-eroding disparities hit certain heritage populations hardest, preying on those in Medicaid-bound, deprived neighborhoods.
The corporate interests promoting legalization profit from both dynamics. Special interests and self-serving behavior shape markets and regulations [10], producing systematic exploitation of at-risk groups. The iron triangle of anti-legalization interests—moralists, commercial interests with stakes in drug treatment and medical marijuana, and law-enforcement entities sustained by the drug war—has been disrupted [10]. A new power structure stands in its place where commercial marijuana interests form a marijuana lobby that may impede public health protections while changing the subject from the harms of criminalization to the harms of corporate predation [10].
Daily marijuana use is associated with a 3.6-fold increase in nicotine dependence [2]. Co-use of marijuana and tobacco is common and affects attempts to quit either substance [2]. From 18% to 39% of adults who used tobacco in the past month also used marijuana, and 69% to 78% of marijuana users used tobacco in the past month [2]. This coincidence creates a population trapped in polysubstance dependence, unable to break free from chemical chains that compromise their judgment, vitality, and capacity for spirited action.
The regulatory incoherence that results from conflicting interest-group politics produces overregulation and misregulation rather than systematic protection of public health [10]. Since policymakers traverse complex lobbying pressures, they create systems that serve corporate interests as they fail to address the fundamental question: who benefits when our youth consume substances that precede psychotic and bipolar disorders by years, that shrink developing brains, and that replace the alertness of nicotine with the passivity of THC?
Our ancestry faces dulling while elites prosper from the cannabis market, extracting wealth through taxes and sales, while our young warriors lose the spiritedness needed to defend territory, heritage, and sovereignty. The trends showing cannabis overtaking cigarettes signal not progress but submission, not liberation but a more sophisticated form of control that operates through commercial temptation rather than legal prohibition.
IV. Constitutional Counterstrike: Policy and Founders’ Mandate
President Trump’s executive order directing marijuana reclassification from Schedule I to Schedule III amounts to a significant federal policy shift, yet it falls catastrophically short of what our threatened bloodline requires [11]. The order directs the attorney general to complete the rulemaking process moving cannabis to Schedule III, alongside ketamine and anabolic steroids, a step that acknowledges medical uses while continuing federal prohibition on recreational consumption [11]. Notwithstanding this advance in recognizing state sovereignty under the 10th Amendment, the reclassification does nothing to address the core crisis: high-potency THC products exceeding 20% concentration, with concentrates reaching 95%, continue flooding markets and doubling psychosis risks in our youth.
To truly protect our youth and heritage, it will take more than federal classification changes. Activists and concerned citizens must exert organized pressure on state and federal lawmakers to demand bold action. Direct tactics include: Flooding legislators’ offices with coordinated phone calls demanding strict THC potency caps; organizing public comments at town halls and legislative hearings; drafting and submitting petitions signed by local coalitions of parents, educators, and health professionals; running letter-writing and email campaigns targeting key committee chairs; creating alliances with existing youth health advocacy groups to amplify demands; and calling on local leaders to issue public statements for urgent regulation. By combining persistent communication with visible public demonstrations and alliance-building, activists can make it politically impossible for politicians to ignore the vital need for real safeguards and swift intervention. Every contact and public demand increases the pressure for a ban on high-potency products, youth marketing, and a true counterattack against corporate interests profiting from adolescent brain harm.
Trump’s Schedule III reclassification is a 10th Amendment victory, but demand more: potency caps, youth marketing bans, and the preservation of Bruen’s 2A for sober defenders.
The 10th Amendment states that powers not delegated to the United States by the Constitution remain reserved to the states or the people. This principle protects state cannabis regulation laws from federal preemption, as the Supreme Court confirmed in 2018 when it struck down the federal PASPA law that sought to prohibit states from authorizing sports gambling, noting it violated the anticommandeering rule [12]. The Court explained that such federal overreach is “as if federal officers were installed in state legislative chambers and were armed with the authority to stop legislators from voting on any offending proposals” [12]. Federal law cannot force states to duplicate or enforce federal policies, and the Department of Justice has never alleged in court that federal laws preempt state medical marijuana or legalization laws [12].
This constitutional framework allows states to serve as laboratories of democracy, but it also permits them to implement protections that Washington refuses to mandate. Because of the potential harm cannabis use poses to youth, many states place restrictions on cannabis advertising, which courts have upheld as constitutional when properly scoped to protect children’s health [13]. Take the case of comprehensive state measures: advertising or marketing placed in broadcast, cable, radio, print, and digital communications can only be displayed where at least 71.6% of the audience is reasonably expected to be 21 years of age or older [4]. Licensees cannot include images of any person or fictional character under 21, must avoid cartoons, and cannot use packaging that imitates products typically marketed to children [4].
Marijuana advertising should not be allowed on television or radio, even within programs ostensibly targeted at adult audiences, as voluntary industry standards have shown insufficient to limit youth exposure [7]. The recently introduced SAFE Advertising Act would permit radio and television stations to accept marijuana advertising if at least 70% of their audience is 21 years old or older, but this threshold is insufficient and difficult to enforce, leaving far too many youth exposed to harmful marijuana messaging [7].
Colorado has pioneered potency regulation through labeling systems designed to help consumers understand THC concentration. Under proposed legislation, producers would be required to use colored strips: blue for THC potency below 5%, yellow for 5% to 15%, orange for 15% to 50%, and red for 50% or more [14]. The proposal initially sought to cap potency levels for buyers 25 or younger but faced pushback, revealing that the industry sells almost all high-potency products to young people aged 21 to 25 [14]. The act prohibits medical marijuana advertising specifically directed to persons aged 18 to 20 years old and limits medical marijuana concentrate purchases to 8 grams per day, or 2 grams for patients 18 to 20 years old [15].
Fellow Warriors of the Founding Blood, true Ethnic Americans whose unyielding European heritage erected this God-blessed Republic under the eternal shield of our sacred Constitution, now is the hour to rise and reclaim our progeny from the globalist dope tyranny! Armed with the 2026 JAMA thunder exposing high-THC weed doubling psychosis and bipolar perils in our youth, sapping their thymos as Plato warned and Raw Egg Nationalist prophesied in “One Nation Under Pot,” we must channel our outrage into firm actions: This week, contact at least three state legislators to demand THC potency caps below 15 percent and strict enforcement against youth marketing. Share this fact-based warning with your local parent groups, and urge school boards to include high-potency cannabis risks in drug education curricula. Specific, measurable action—taken by each of us—can shield our children’s future. Let us advance not only in spirit, but in deed.
The Supreme Court’s decision in New York State Rifle & Pistol Association Inc. v. Bruen revolutionized Second Amendment doctrine in June 2022, directing courts to draw analogies from history rather than apply interest-balancing tests [16]. Since Bruen, lower courts have struck down various modern gun laws, creating unpredictable outcomes [16]. The connection to cannabis policy appears through the requirement for sober, vigilant defenders capable of exercising their constitutional rights. Cannabis arrests brain development and creates populations less capable of the judgment and reaction time necessary for responsible firearms ownership.
1790 Naturalization Act: Preserve the White Republic—reject federal overreach clashing with state rights, shield our blood from “benign” myths.
The Naturalization Act of 1790 set the first uniform rules for granting United States citizenship by naturalization, limiting it to “free white person(s)…of good character” [17]. This law eliminated ambiguity on how to treat newcomers and required a two-year residency in the United States and one year in the state of residence before an alien could apply for citizenship [17]. Congress modeled the act on the British Parliament’s Plantation Act of 1740 and established that once convinced of the applicant’s good character, the court would administer an oath of allegiance to support the Constitution [17].
The act provided that children born abroad when both parents are US citizens “shall be considered as natural born citizens,” specifying that citizenship rights did “not descend to persons whose fathers have never been resident in the United States” [17]. Congress amended the naturalization law in 1795, requiring an applicant to submit a declaration of intent at least 3 years before naturalization and extending the minimum residence requirement to 5 years [18]. In 1802, Congress restored both the five-year residence requirement and the three-year declaration period, establishing patterns that continued for decades [18].
This founding framework understood that citizenship carries obligations of character and allegiance. In order that we preserve the constitutional republic against threats both foreign and domestic, we must recognize how substances that precede psychiatric diagnoses by years, shrink developing brains, and replace alertness with passivity undermine the capacity toward self-governance the Founders envisioned. The question of federal versus state authority over cannabis parallels debates over naturalization: who decides the standards by which our communities function and who belongs within them?
Big Weed’s blitz as tyranny against liberty, exacerbating disparities per Gallup/Pew.
The marijuana industry spent over $4.2 million lobbying on various issues and legislation in 2021, including the Marijuana Opportunity, Reinvestment and Expungement Act [5]. Organizations spent a combined $31.1 million lobbying in 2021 on issues including the MORE Act [5]. In 2025, the industry spent $4,855,500 with 19 clients and 71 lobbyists, of whom 50.7% were former government employees [19]. The National Cannabis Industry Association spent $150,000 on two lobbyists between April and December 2021 [5].
This lobbying apparatus operates as tyranny against liberty, using concentrated financial means to direct policy that damages public health while enriching corporate interests. Undoubtedly, the pattern replicates tobacco and alcohol industry strategies that harmed many young people through commercialization that normalized use, increased exposure and access, and emboldened the industry to target young users [7].
Public opinion polling reveals the manipulation underlying these efforts. Seven in 10 Americans think marijuana use should be legal, the highest level yet, with 29% opposed and 1% unsure [3]. Support cracked the 50% threshold in 2013, jumping 10 percentage points to 58% after Colorado and Washington legalized recreational use [3]. As of 2024, support for legalization is highest among self-identified liberals at 91% and Democrats at 87%, lowest among conservatives at 52% and Republicans at 55% [3].
The vast majority of Americans support legalizing marijuana in some way, with around nine-in-ten adults saying either that marijuana should be legal for medical and recreational use at 54% or for medical use only at 33% [20]. Another 12% say the drug should not be legal at all [20]. Republican support for legalization fell 13 percentage points over the past year, down to 40%, the lowest level among this group in a decade [21]. This decline shows improved Republican perceptions under Trump and his aggressive actions to limit drug entry [21].
Those disparities in support correlate with the ethnic-eroding patterns documented in usage data, where socioeconomically advantaged groups consume cannabis while disadvantaged populations face greater consequences. The polling shows 70% support in both states where recreational use is legal and states with restrictive laws [3], suggesting corporate propaganda has succeeded in normalizing a substance that doubles psychosis risks regardless of jurisdiction. On condition that we protect our heritage and constitutional liberties, we must recognize Big Weed’s lobbying blitz as an assault on the sovereignty and spiritedness our Republic requires for survival.
V. Rally the Bloodline: Call to Mobilization and Vision Forward
The evidence stands irrefutable: high-THC cannabis doubles psychosis risk in our youth, shrinks developing brains, and operates as a corporate weapon that saps the thymos our Republic just needs. We’ve armed you with 2026 JAMA thunder-tracking data on 463,396 teens and Dr. Amen’s brain scans. Raw Egg Nationalist warns that weed replaces nicotine’s watchfulness with passive submission. Trump’s Schedule III move honors the 10th Amendment. Yet we must just need potency caps and youth marketing bans.
Now is the time to move from isolated concern to united, broad-based action. Join the crusade alongside educators, parent groups, medical professionals, veterans organizations, youth mentors, and all who defend our community’s future. Connect and build strong coalitions with groups already working to protect youth mental health, fight addiction, and preserve civic vitality. Framing this fight as a collective stand for the health and toughness of our people will generate unstoppable momentum.
Share this exposé on X and tag @realDonaldTrump, @TuckerCarlson, @DrDanielAmen, and @elonmusk. Launch polls asking “Ban High-THC Poison?” Petition representatives to secure constitutional protections that guard our heritage’s destiny against globalist dope tyranny!
FAQs
Q1. How does cannabis use during adolescence affect the risk of developing mental health disorders? Research tracking over 460,000 adolescents found that past-year cannabis use during ages 13-17 was associated with more than double the risk of developing psychotic disorders (2.19 times) and bipolar disorder (2.0 times) by age 26. Cannabis use preceded these psychiatric diagnoses by an average of 1.7 to 2.3 years, and the risk increases with today’s high-potency products containing THC levels exceeding 20%, compared to 2-4% in previous decades.
Q2. What are the effects of cannabis use on the developing teenage brain? Cannabis use during adolescence is associated with accelerated cortical thinning, particularly in the prefrontal cortex, which controls executive functioning and doesn’t fully develop until around age 25. Studies show THC causes shrinkage of dendritic connections between neurons, resulting in long-lasting decrements in IQ, working memory, decision-making, attention, and academic performance. Brain imaging reveals abnormally low blood flow in nearly every brain region studied among marijuana users.
Q3. Can cannabis use during pregnancy harm the developing baby? Yes, THC crosses the placenta and transfers into breast milk, attaining approximately 10% of maternal concentration in the fetus. Prenatal cannabis exposure has been linked to low birth weight, premature birth, and NICU admission. Long-term effects include increased risk of attention deficit disorders, behavioral problems, memory challenges, and altered gene expression associated with autism spectrum disorder and ADHD, with effects differing between male and female offspring.
Q4. What is the connection between cannabis use and increased dementia risk? Emergency room visits or hospitalizations due to cannabis use are associated with a 72% increased risk of dementia diagnosis within five years. Research shows marijuana use causes abnormally low blood flow in brain regions affected by Alzheimer’s disease, especially the hippocampus, which is critical for forming memories. Long-term heavy cannabis use has been linked to memory problems in midlife and structural brain changes associated with dementia.
Q5. How have THC potency levels changed in modern cannabis products? Modern cannabis products contain dramatically higher THC concentrations than in previous generations. Average THC content in cannabis flower now exceeds 20%, compared to 2-4% decades ago. Concentrated products can contain 70-95% THC, delivering far more potent doses that act on cannabinoid receptors highly expressed in the adolescent brain, significantly increasing risks for adverse mental health outcomes and neurodevelopmental disruption.
References
[1] – https://www.marijuanamoment.net/more-americans-now-use-marijuana-than-smoke-cigarettes-new-study-shows/
[2] – https://www.cdc.gov/pcd/issues/2020/20_0110.htm
[3] – https://news.gallup.com/poll/514007/grassroots-support-legalizing-marijuana-hits-record.aspx
[4] – https://www.cannabis.ca.gov/posts/cannabis-products-attractive-to-children-prohibited/
[5] – https://www.opensecrets.org/news/2022/04/the-marijuana-industry-spent-millions-lobbying-on-legalization-in-2021/
[6] – https://addictionpolicy.stanford.edu/making-legalized-marijuana-production-and-sale-non-profit-protect-public-health
[7] – https://drugfree.org/article/protect-youth-from-harmful-marijuana-advertising/
[8] – https://ask.usda.gov/s/article/askFSIS-Public-Q-A-Hemp-as-an-Ingredient-in-Meat-Poultry-and-Egg-Product
[9] – https://www.cdc.gov/mmwr/volumes/74/wr/mm7412a1.htm
[10] – https://www.brookings.edu/articles/bootleggers-baptists-bureaucrats-and-bongs-how-special-interests-will-shape-marijuana-legalization/
[11] – Owens, M. M., et al. (2022). Bayesian causal network modeling implies adolescent cannabis use accelerates prefrontal cortical thinning. Transl Psychiatry 12(1). https://doi.org/10.1038/s41398-022-01994-0
[12] – Ryan, K. S., Karpf, J. A., Chan, C. N., Hagen, O. L., McFarland, T. J., Urian, J. W., Wang, X., Boniface, E. R., Hakar, M. H., Terrobias, J. J., Graham, J. A., Passmore, S., Grant, K. A., Sullivan, E. L., Grafe, M. R., Saugstad, J. A., Kroenke, C. D. & Lo, J. O. (2024). Prenatal delta-9-tetrahydrocannabinol exposure alters fetal neurodevelopment in rhesus macaques. Scientific Reports 14. https://doi.org/10.1038/s41598-024-56386-7
[13] – Thakrar, A. & Rastegar, D. A. (August 26, 2021). THC Concentration in Cannabis Increased Worldwide Between 1970 and 2017. Alcohol, Other Drugs, and Health: Current Evidence. https://www.bu.edu/aodhealth/2021/08/27/thc-concentration-in-cannabis-increased-worldwide-between-1970-and-2017/
[14] – Rotering, T. & Apollonio, D. E. (2022). Cannabis Industry Lobbying in the Colorado State Legislature in 2010–2021. International Journal of Drug Policy 102. https://doi.org/10.1016/j.drugpo.2022.103585
[15] – (2026). Longitudinal trends in the past 30-day co-use of nicotine/tobacco, alcohol, and cannabis among youth and adults in the PATH study. Addictive Behaviors 108. https://doi.org/10.1016/j.addbeh.2026.108633
[16] – Eser, A. (2026). Adolescent Substance Abuse: ZipDo Education Reports 2026. ZipDo Education Reports. https://zipdo.co/adolescent-substance-abuse-statistics/
[17] – (NIDA), N. I. (December 11, 2024). Reported use of most drugs among adolescents remained low in 2024. NIDA. https://nida.nih.gov/news-events/news-releases/2024/12/reported-use-of-most-drugs-among-adolescents-remained-low-in-2024
[18] – Large, M., Sharma, S., Compton, M. T., Slade, T. & Nielssen, O. (2011). Cannabis use and earlier onset of psychosis: a systematic meta-analysis. Archives of General Psychiatry 68(6), pp. 555-561. https://doi.org/10.1001/archgenpsychiatry.2011.5
[19] – Hines, L. A., Freeman, T. P., Gage, S. H., Zammit, S., Hickman, M., Cannon, M., Munafo, M., MacLeod, J. & Heron, J. (2020). Association of High-Potency Cannabis Use With Mental Health and Substance Use in Adolescence. JAMA Psychiatry 77(10), pp. 1044-1051. https://doi.org/10.1001/jamapsychiatry.2020.1035
[20] – Aks, I. R., Patel, H., 3rd, W. E., Huestis, M. A., & Wade, N. E. (2025). Cannabinoids in hair and their prospective association with mental and physical health outcomes in adolescents. Neurotoxicology and Teratology 108. https://doi.org/10.1016/j.ntt.2025.107433
[21] – (2007). Cannabis Use and Earlier Onset of Psychosis: A Systematic Meta-analysis. JAMA Psychiatry 64(4), pp. 480-487. https://doi.org/10.1001/archpsyc.64.4.480
[22] – Hines, L. A., Cannings-John, R., Hawkins, J., Bonell, C., Hickman, M., Zammit, S., Adara, L., Townson, J. & White, J. (2024). Association between cannabis potency and mental health in adolescence. Drug Alcohol Depend. 2024;261:111359.. https://doi.org/10.1016/j.drugalcdep.2024.111359
[23] – (n.d.). European Drug Report 2025: Trends and Developments. https://www.euda.europa.eu/publications/european-drug-report/2025/cannabis_en
[24] – (December 16, 2024). Reported Drug Use Among Adolescents Remained Low in 2024. National Institute on Drug Abuse. https://nida.nih.gov/news-events/news-releases/2024/12/reported-use-of-most-drugs-among-adolescents-remained-low-in-2024
[25] – (2025). A Fine-Grained Longitudinal Study of Adolescent Cannabis Use and Its Relation to Cognitive Performance in Young Adulthood. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-025-01604-0
[26] – Albaugh, M. D., Ottino-González, J., Sidwell, A. et al. (2021). Association of Cannabis Use During Adolescence With Neurodevelopment. JAMA Psychiatry 78(9), pp. 1036-1045. https://doi.org/10.1001/jamapsychiatry.2021.1258
[27] – Tamnes, N., Østby, S., Fjell, S., Westlye, A., Due-Tønnessen, A. & Walhovd, A. (2010). Developmental Trajectories of Cortical Thickness Across the Lifespan. Cerebral Cortex 20(3), pp. 534-548. https://doi.org/10.1093/cercor/bhp118
[28] – Tadesse, A. W., Dachew, B. A., Ayano, G., Betts, K. & Alati, R. (2024). Prenatal cannabis use and the risk of attention deficit hyperactivity disorder and autism spectrum disorder in offspring: A systematic review and meta-analysis. Journal of Psychiatric Research 171, pp. 142-151. https://doi.org/10.1016/j.jpsychires.2024.01.045
[29] – Sarikahya, M. H., Cousineau, S. L., Felice, M. D., Szkudlarek, H. J., Wong, K. K., DeVuono, M. V., Lee, K., Rodríguez-Ruiz, M., Gummerson, D., Proud, E., Ng, T. H., Hudson, R., Jung, T., Hardy, D. B., Yeung, K. K., Schmid, S., Rushlow, W. & Laviolette, S. R. (2023). Prenatal THC exposure induces long-term, sex-dependent cognitive dysfunction associated with lipidomic and neuronal pathology in the prefrontal cortex-hippocampal network. Schizophrenia Bulletin 49(5), pp. 4234-4250. https://doi.org/10.1038/s41380-023-02190-0
[30] – (2024). Cannabis and Secondhand Smoke. Centers for Disease Control and Prevention. https://www.cdc.gov/cannabis/health-effects/secondhand-smoke.html\
[31] – https://www.infowars.com/posts/teenage-cannabis-use-doubles-risk-of-psychotic-and-bipolar-disorders
[32] – https://medicalxpress.com/news/2026-02-adolescent-cannabis-linked-psychotic-bipolar.html
[39] – https://x.com/Babygravy9/status/1842111944058102050?s=20
[40] – https://x.com/Babygravy9/status/1991157205358289122?s=20
[41] – https://x.com/TuckerCarlson/status/1990490136220430632?s=20
[45] – https://www.foxnews.com/category/person/donald-trump
[46] – https://www.foxnews.com/health/using-marijuana-cope-stress-trauma-may-backfire-studies-warn
[48] – https://www.foxnews.com/category/health/mental-health/psychosis
[50] – https://www.foxnews.com/health/fatal-crash-report-finds-nearly-half-deadly-wrecks-tied-illegal-drug
[51] – https://www.youtube.com/watch?v=fAe8He-Qca8
[53] – https://www.foxnews.com/category/media
[55] – https://www.amazon.com/Tell-Your-Children-Marijuana-Violence/dp/1982103671
[56] – https://www.foxnews.com/category/health/mental-health/addiction
[57] – https://counter-currents.com/2017/07/white-nationalism-is-american-nationalism/
[61] – https://x.com/MarinaMedvin/status/1705028446840037588
[62] – https://sites.harvard.edu/sitn/
[63] – https://www.pnas.org/doi/10.1073/pnas.1920325116
[64] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3930618/
[66] – https://www.aei.org/op-eds/no-amount-of-marijuana-is-safe-for-teens/
[67] – https://thehill.com/opinion/healthcare/5347506-the-case-for-restricting-cannabis-age/

Leave a comment